

Being Female Is Not a Disease: The Untapped Investment Opportunity in Women’s Health
From hysteria to antidepressants, medicine has long medicalized women’s distress instead of solving it. Here’s why that blind spot is also a trillion-dollar opportunity.


This newsletter is free. But it takes hours each week to research, write, and produce at this level. Here are 5 ways to support my work: 1. click “❤️” to amplify 2. subscribe 3. share this publication 4. buy me coffee 5. become a partner
Connect and collaborate with me here! Email | LinkedIn | Instagram
In the late 1800s, doctors had a word for women’s pain. They called it hysteria.
A catchall diagnosis for anything that didn’t fit neatly into the medical textbooks of the time: fatigue, headaches, abdominal cramps, mood swings, even grief. If a woman cried too much or asked too many questions, hysteria was invoked. The prescription was often rest cures, isolation, or worse, institutionalization. Care was less about healing and more about silencing.
By the 1950s, the word had fallen out of fashion. But the logic remained. Doctors wrote millions of prescriptions for tranquilizers - the so-called “mother’s little helpers.” Advertisements showed smiling housewives holding pill bottles, as if sedation were the cure for the impossible demands of perfection. Anxiety, exhaustion, and the psychic weight of gendered expectations were medicalized into chemical management.
And now, after 2020, the data reveal another sharp turn in the same story. In the United States, monthly antidepressant dispensing for girls aged 12–17 increased 129.6% faster than prior trends after the onset of COVID-19, while rates for boys declined during the same period1.
Every era medicalizes female distress. Every era calls it care.

New Here?
If you are an investor, operator, or women’s health advocate, start here.
→ Preorder the book: The Billion Dollar Blind Spot
→ Subscribe to the podcast: Blindspot Capital
→ Join the FemmeHealth Alliance Circle
The Hidden Bias in Women’s Health
Medicine struggles with what it cannot measure. When a woman reports chronic fatigue, or monthly pain that doesn’t show up on a scan, the system has little to hold onto.
The default response has been the prescription pad. Treat the symptom, not the source. Quiet the patient, not the problem.
This isn’t coincidence. Convenience shapes science, and capital follows convenience. Women are consistently more likely than men to be prescribed psychotropic medications, including antidepressants and anxiolytics23.
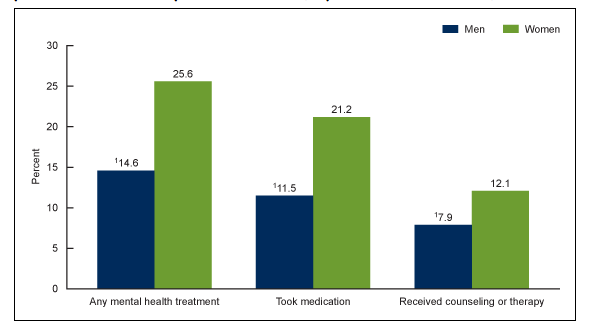
At the same time, women’s access to therapy or non-drug interventions is uneven, with data showing they are significantly more likely to use medication for mental health than men4.
Blockbuster drugs get the funding. Reimbursement flows to what’s already on the shelf. And so the cycle repeats: sedation over solutions.
How Bias Shapes Women’s Mental Health, Endometriosis, and Menopause Care
You can see the traces everywhere.
In psychiatry, where women are about 1.5–2 times more likely than men to be prescribed psychotropic medication.
In reproductive health, where conditions like endometriosis still take an average of 7–8 years to diagnose in high-income countries, leaving millions managed with painkillers or hormonal contraceptives rather than targeted therapies5.
In menopause, where decades of fear around hormone therapy inflamed by the misinterpreted Women’s Health Initiative (WHI) study of 2002 have left large numbers of women untreated, despite evidence that appropriately prescribed hormone therapy can reduce risks for osteoporosis and, in some cases, cardiovascular and cognitive decline6.
This is the legacy of a system that confuses sedation with care. A system that narrows its definition of treatment to what can be written on a prescription pad, leaving prevention, precision, and lived experience outside the frame.
But the truth every investors should hear is this: every time the system defaults to a prescription, it leaves the harder and more valuable problems unsolved.
❤️ Enjoying this? If this post sparked something for you, click the ❤️ at the bottom. It helps more than you know and tells me you're reading.
Meet the Founders Redefining Women’s Health Innovation
For decades, women with endometriosis were told the same line: “take painkillers until you want children.” Diagnosis required surgery, so most were left untreated.
Somer Baburek refused that script. At Hera Biotech, she is developing a non-surgical diagnostic to finally give women answers and with them, options7.
She’s not alone. Hadas Ziso at Endocure is building an accurate, non-invasive test to end the eight-year diagnostic delay.
And Sabrina Johnson at Daré Bioscience has pushed forward products in contraception, menopause, and sexual health, precisely the spaces big pharma abandoned.
Each is a refusal to accept sedation as care. Each reframes women’s health as a frontier of science, not a footnote.
Why Women’s Health Is the Most Overlooked Investment Opportunity
Investors often ask me: Where is the real opportunity in women’s health? The answer is here, in the blind spots medicine keeps writing off.
The antidepressant prescription curves are not just clinical data. They are economic signals. They reveal markets that rely on managing symptoms instead of addressing causes. They expose the opportunity to build therapies, technologies, and platforms that deliver real solutions.
Being female is not a disease. It is the most overlooked investment opportunity of our time.
The investors who see that won’t just back better science. They will rewrite the future of care and claim the value history has been too blind to measure.
P.S. In a few weeks we’ll be opening membership for the FemmeHealth Alliance, a new non-profit platform to connect capital, science, and policy for women’s health. If you’d like to be among the first to join, link here.
If this essay moved you, share or restack it.
This essay is part of my ongoing series on the billion-dollar blind spot in women’s health, wealth, and capital. You can subscribe to receive new essays every Sunday and join the conversation shaping the future of investing
To go deeper, pre-order my upcoming book The Billion Dollar Blind Spot to learn why women’s health is the future of healthcare investing.
Join Our Network
Are you building or backing credible, under-the-radar solutions in women’s health?
We want to hear from you. Reach out privately or reply to this post. FHV curates brands and breakthroughs that deserve broader attention in the women’s health ecosystem.
I write weekly at FemmeHealth Ventures about capital, care, and the future of overlooked markets. If you are building, backing, or allocating in this space, I’d love to connect.
Disclaimer & Disclosure
This content is for informational and educational purposes only. It does not constitute financial, investment, legal, or medical advice, or an offer to buy or sell any securities. Opinions expressed are those of the author and may not reflect the views of affiliated organisations. Readers should seek professional advice tailored to their individual circumstances before making investment decisions. Investing involves risk, including potential loss of principal. Past performance does not guarantee future results.
References
Anderson KN, et al. Antidepressant Dispensing to US Adolescents and Young Adults Before and During the COVID-19 Pandemic. Pediatrics. 2024;153(3):e2023064245
Abbing-Karahagopian V, et al. Gender differences in psychotropic medication use in Europe. European Psychiatry. 2015;30(6):778-788.
Estancial Fernandes CS, de Azevedo RCS, Goldbaum M, Barros MBA. Psychotropic use patterns: Are there differences between men and women? PLoS One. 2018 Nov 26;13(11):e0207921. doi: 10.1371/journal.pone.0207921. PMID: 30475871; PMCID: PMC6257918.
Terlizzi EP, Norris T. Mental Health Treatment Among Adults: United States, 2020. NCHS Data Brief, no 419. National Center for Health Statistics. 2021.
Fuldeore MJ, Soliman AM. Prevalence and Symptomatic Burden of Diagnosed Endometriosis in the United States: National Estimates from a Cross-Sectional Survey of 59,411 Women. Gynecol Obstet Invest. 2017;82(5):453-461.
Manson JE, Kaunitz AM. Menopause management — getting clinical care back on track. N Engl J Med. 2016;374(9):803-806.
Keep up the good work.. not always easy in the face of ignorance and greed.. yet you are loved and respected and appreciated
Without reading this, I can already predict what’s coming. I’ve worked in places where it seems all women have a negative association with their biology, including hormonal issues, painful periods, PMS, anxiety/depression, and So. Many. Hysterectomies. A rabbit hole ensues.